Flap Transplantations
|

|
Maxillofacial Surgery 
Flap Vascularisation
A revision of flaps is still necessary in 12-17% of flap transplantations, mainly due to
vascular thrombosis. Therefore, as a diagnostic aid, the laser Doppler device
had been used recently [1]. But the problems for pure blood flow measurements
were the diagnosis of venous congestions.
With O2C venous congestions can be distinguished from arterial occlusions and
oxygen utilisation problems can be identified.
Flap regions can be examined with regard to its oxygen supply qualities and
blood supply development can be observed over time. [2].
The figure at the right side of this picture shows varied oxygen saturations
of different donor sites [3].
Below, you can see exemplary perfusion parameters of different points of a TRAM
flap.
Maxillofacial Surgery
Continuous
observation of blood and oxygen supply of flaps result in increased safety during
transplantations in maxillofacial surgery.
Flap Vascularisation
Tissue
blood supply after transplantation of a pedicled flap- microcirculation two
days and one week after surgery and flap conditioning
Viability
of tissue of a transplanted flap requires sufficient perfusion and supply with
oxygen. In pedicled flaps blood in- and outflow to and from the recipient site
is therefore sustained by the vessels of the donor site until new vessels grow
into the flap. By flap conditioning (pinching off the blood inflow from the
donor site) stimuli are set, that accelerate growth of new vessels from the
recipient site. If the flap tolerates the occlusion of the pedicle for 2 hours,
it is disconnected (mostly after 3 weeks). Then blood supply only takes place
through the newly grown vessels of the recipient site.
In the
shown case a big defect of the soft part of the hand was covered by a pedicled
groin flap. A few days after surgery flap training was started. At the 2. and
9. day of flap conditioning the blood flow, oxygen saturation and hemoglobin
amount were measured by the probe before, during and after occlusion of the
flap pedicle.
Tissue neovascularisation two days after transplantation
After two
days oxygen saturation, blood flow and hemoglobin amount decreases clearly during
occlusion of the supplying vessel. During occlusion an increase of hemoglobin
amount occurs, caused by a venous congestion of the faster occlusion of the
vein. After the occlusion there is reactive hyperemia, that lasts for 5 minutes
until values return to baseline. During reactive hyperemia particularly blood
flow increases highly above baseline values. Vessel dilatation and higher venous
filling can be observed by local hemoglobin amount.

[click on figure to maximize]
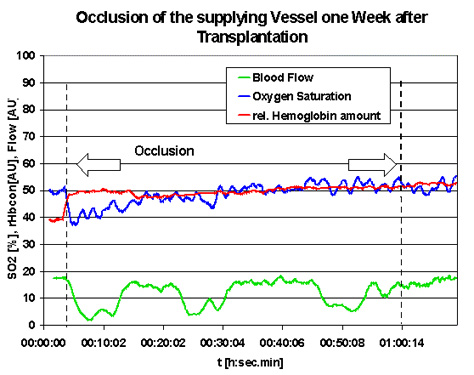
Tissue neovascularisation one week after transplantation
One week after transplantation perfusion is almost stable after occlusion of the abdominal vessel. Oxygen saturation only decreases by a few percent. The small increase
of hemoglobin amount indicates a small outflow problem, during occlusion of
abdominal vessels.
[click on figure to maximize]
The small
increase of all parameters during measurement period indicates a warming of
the hand, that can be explained by the blanket with which the hand was covered
during the whole measurement.
Interestingly
there are high variations of the blood flow during occlusion for relative long
time periods (about 5 minutes). During those strong decreases pulsation of the
blood flow could be observed the whole time. As this decrease of perfusion has
almost no influence on oxygen saturation, there is a change in oxygen uptake
of the measured tissue. This can be caused by a change of metabolism of the
cells, which usually shows slower dynamics, or by a redistribution of the blood
from nutritive vessels to e.g. shunt vessels.
With O2C
blood supply and important hemodynamic conditions of transplanted tissues can
be characterized by determination of the parameters of microcirculation: oxygen
saturation, blood flow and hemoglobin amount. The diagnosis of flap hemodynamic
conditions includes discrimination of undersupply by arterial or venous occlusion,
decrease of oxygen uptake by decreased metabolism or shunt perfusion and successful
neovascularisation.
This
examination was performed together with:
Prof. Dr. Lanz, Klinik f. Handchirurgie, Herz- und Gefäßklinik GmbH,
Bad Neustadt
Literature:
O2C
Papers
- Long-term
physical activity and neurologic function after harvesting of the radial artery as Tgraft
or free graft in coronary revascularization.
K. Knobloch, A. Lichtenberg, S. Tomaszek, C. Hagl, N. Khaladj, U. Klima, A. Haverich;
Ann Thorac Surg. 2005 Sep;80(3):918-21
- O2C relevant data extracted from
"Palmar Microcirculation After Harvesting of the Radial Artery in
Coronary Revascularization"
- Simultanes nichtinvasives
Monitoring mit Laser-Doppler-Flussmessung und Gewebespektrometrie bei fasziokutanen Radialislappen
und osteokutanen Fibulatransplantaten
F. Hölzle, A. Rau, S. Swaid, D. J. Loeffelbein, D. Nolte, K.-D. Wolff;
Mund-, Kiefer- und Gesichtschirurgie 2005 Sep;9(5):290-9,
ISSN: 1432-9417 (Paper) 1434-3940 (Online), DOI: 10.1007/s10006-005-0636-2
- Simultaneous noninvasive
monitoring for radial forearm and fibula flaps using laser Doppler flowmetry and tissue
spectrophotometry.
F. Hölzle, A. Rau, S. Swaid, D. J. Loeffelbein, D. Nolte, K.-D. Wolff;
Mund-, Kiefer- und Gesichtschirurgie 2005 Sep;9(5):290-9
- Laser-doppler-flowmetry and absorption-tissue-spectrometry of the transposed groin flap - A comprehensive and independent analysis of microcirculation
K. Wolf, E. Höcherl, T. Derfuß, A. Krug; Applied Cardiopulmonary Pathophysiology ll: 000-000, 2003
- Nutritive perfusion at donor site after microvascular fibula transfer
Holzle F, Swaid S, Nolte D, Wolff KD.; Microsurgery. 2003
- POSTER: Combined
Non-Invasiv Tissue Oxygen and Flow Monitoring in Fasciocutaneous Forearm Flaps
- Non-invasive tissue oxygen monitoring in fasciocutaneous flaps
Hölzle F, Löffelbein D., Swaid S.; J. Cranio Maxill Surg. (2002) 30, Supplement 1:108
- O2C relevant data extracted from "O2C (oxygen to see) values typical/critical for flaps"
- O2C relevant data extracted from "Parameters of Microcirculation and Healing Time of Burn Wounds"
Talks
- Simultaneous non-invasive tissue oxygenation and blood flow monitoring in microsurgical flaps
Hölzle F., Franz E.-P., Swaid S., Nolte D., Wolff K.-D.; XVII. Congress of Cranio-Maxillofacial Surgery, Tours, France, 2004
- Therapeutische Optionen zur Verbesserung der Mikrozirkulation
Dr. J. Hoffmann; 14. Symposium Intensivmedizin / Intensivpflege, Bremen, 18.-20.02.2004
- Simultanes noninvasives Monitoring von Hämoglobin, Hämoglobin-Oxygenierung, Blutfluss und Blutflussgeschwindigkeit bei mikrochirurgischen Transplantaten
Hölzle F., Rau A., Swaid S., Nolte D., Wolff K.-D.; 53. Kongress der deutschen Gesellschaft für Mund-, Kiefer- und Gesichtschirurgie, Krefeld, 2003
- Hautdurchblutung im Entnahmebereich nach mikrochirurgischem Fibulatransfer
Hölzle F., Watola A., Swaid S., Nolte D., Wolff K.-D.; 40. Kongress der Deutschen Gesellschaft für Plastische und Wiederherstellungschirurgie, Leipzig, 2003
- Noninvasives Monitoring fasziokutaner Unterarmlappen mit simultaner Laser-Doppler-Spektrometrie
Löffelbein D. J., Hölzle F., Rau A., Nolte D., Wolff K.-D.; 40. Kongress der Deutschen Gesellschaft für Plastische und Wiederherstellungschirurgie, Leipzig, 2003
- Laser-Doppler-Flowmetrie (LDF) und Absorptions-Gewebe-Spektrometrie (AGS). Ein Beitrag zur Analyse der Mikrozirkulation am Lappentransponat
Wolf K, Krug A, Sebisch E, Höcherl E; 67. Jahrestagung der Deutschen Gesellschaft für Unfallchirurgie, 89.
Tagung der Deutschen Gesellschaft für Orthopädie und Orthopädische Chirurgie und 44. Tagung des Berufsverbandes
der Fachärzte für Orthopädie. Berlin, 11.-16.11.2003.
- Noninvasives Monitoring bei ischämischer Präkonditionierung eines osteomyocutanen Fibulatransplantates über die A. radialis
Hölzle F., Watola A., Swaid S., Wolff K.-D.; 40. Kongress der Deutschen Gesellschaft für Plastische und Wiederherstellungschirurgie, Aachen, 2002
- Non-invasive
Oxygen and Perfusion Monitoring (Abstract)
A.Krug, Hindsgavl, Danemark, 2002
- Simultaneous
non-invasive Fluxmetry and tissue oxygen Monitoring in fasciocutaneous Flaps
Poster
D. Nolte, J Craniomaxillofac Surg. 2002 Sep
- Donor
Site Morbidity of the osteocutaneous Fibula Flap
Hölzle F, J Craniomaxillofac Surg. 2002 Sep
- The
radial Artery as a carrier of the osteocutaneous Fibula Flap for reconstruction
of the Mandibula
Hölzle F, J Craniomaxillofac Surg. 2002 Sep
Case Studies
Empho
Papers
- Hämoglobin-Oxygenierung der Haut an verschiedenen Spenderregionen für mikrochirurgische Transplantate
Hölzle F, Swaid S, Nolte D, Wolff KD.; Journal DGPW (2002): 25, 17-22
- Cutaneous
hemoglobin oxygenation of different free flap donor sites
K. D. Wolff, A. Kolberg, U. Mansmann;
Ann Plast Surg 1998 Dec;41(6):646-52; discussion 652-3
- Intracapillary haemoglobin oxygenation and interstitial pO2 in venous flaps: an experimental study in rats
KD. Wolff, Microsurgery, 1998
- Hemoglobin oxygenation of venous-perfused forearm flaps
KD Wolff, Ann Plast Surg, 1998
- Monitoring
of flaps by measurement of intracapillary haemoglobin oxygenation with EMPHO II: experimental and clinical study
K. D. Wolff, C. Marks, B. Uekermann, M. Specht, K. H. Frank;
Oral MaxillofacSurg 1996 Dec;34(6):524-9
- Noninvasive intraoperative measurement of intracapillary hemoglobin oxygenation and relative hemoglobin concentration in surgical skin flaps
M. Kasler, HNO, 1990